
I Ranked Every Tesamorelin Seller the Way I’d Rank Them for a Friend Who’s Already Decided

Let’s skip the part where I tell you not to do this. If you’re reading a piece titled with the word “ranked,” you’ve probably already decided tesamorelin is happening. My job isn’t to talk you out of it. My job is to make sure that if you go get it, you go get it in the way that’s least likely to hurt you, and to be straight with you about the parts that no seller, however careful, can fix.
Quick fact-check before anything else: tesamorelin is a real, FDA-approved drug, brand name Egrifta, approved in November 2010 for one specific job, reducing excess abdominal fat in people with HIV-associated lipodystrophy [R3]. That’s it. That’s the whole approved use. Everything past that, general belly-fat loss, anti-aging, growth-hormone chasing, is off-label. Not fake, not necessarily useless, just unproven at the standard the FDA actually checked.
The real risks, named without flinching
Here’s what I want you to sit with before you open a browser tab.
The label warning is not decorative. Tesamorelin’s prescribing information tells clinicians to monitor for changes in glucose metabolism [R3]. That’s not a throwaway line, it’s there because the drug can move your blood sugar. If nobody is checking yours before and during use, that’s a real gap, not a technicality.
IGF-1 goes up, and that has a downstream implication. In the pivotal 26-week trial, IGF-1 rose about 81% in treated patients [R1]. Higher IGF-1 has a theoretical link to tumor growth, which is why anyone with an active or recent malignancy is generally steered away from this drug. If you have that history and a seller never asks, that’s your risk, not theirs.
“Research use only” means exactly what it says. A chunk of this market is powder shipped with a label claiming it’s not for human consumption. That disclaimer exists so the seller can operate outside drug regulation. It also means: no clinician checked your glucose, nobody verified what’s actually in the vial beyond a certificate the seller paid for and chose to publish, and if something goes wrong, there’s no prescriber on record and no pharmacy standard behind the product.
A certificate of analysis is not a safety net. At its best, a COA tells you about identity and purity for one sample. It usually says nothing about sterility or endotoxin levels, which are the things that actually matter when you’re injecting something. And it’s rarely tied to the specific vial landing in your fridge.
If you compete in tested sport, this is a hard no regardless of source. Tesamorelin is a GHRH analogue, and it’s named explicitly on the WADA 2026 Prohibited List under category S2 [R4]. Brand, compound, or gray-market vial, doesn’t matter. No prescription changes this.
That’s the risk picture, unvarnished. Now let’s talk about lowering it as much as it can be lowered.
What the evidence actually earns, so you know what you’re extrapolating from
I’m not going to pretend the drug is fake or that the research doesn’t exist, because it does, and it’s decent.
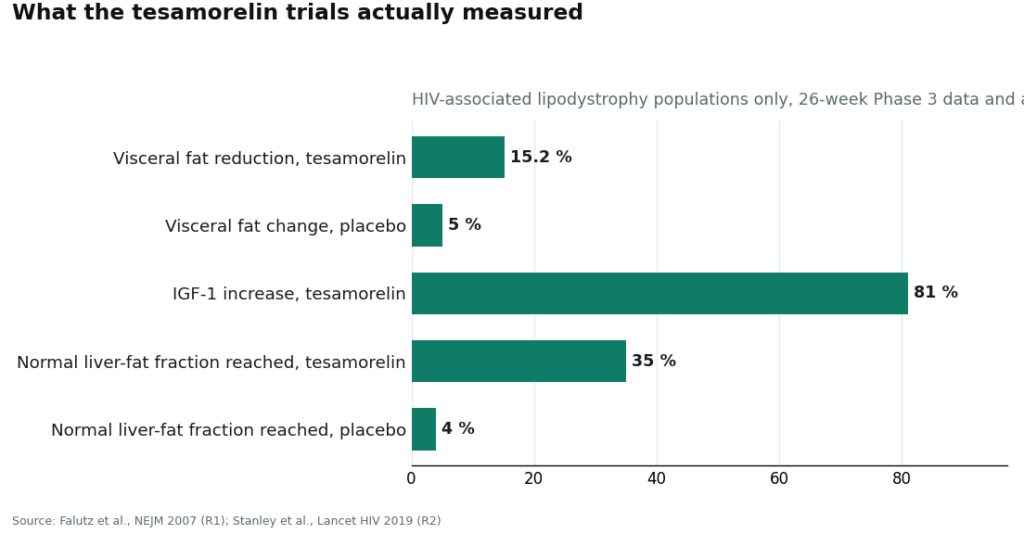
The Phase 3 trial that got Egrifta approved randomized 412 people with HIV-related lipodystrophy to 2 mg daily tesamorelin or placebo for 26 weeks. Visceral fat dropped 15.2% in the treated group versus a 5.0% increase on placebo, triglycerides improved, and IGF-1 rose about 81% [R1]. A follow-up Lancet HIV trial in 2019 found tesamorelin reduced liver fat too, with about 35% of treated patients hitting a normal liver-fat fraction versus 4% on placebo [R2].
Those numbers are real and they’re solid by peptide standards. But every single one of them came from people with HIV-associated lipodystrophy. If that’s not you, and for most people buying tesamorelin online, it isn’t, you are extrapolating from evidence gathered in a different population. That’s not automatically wrong. It’s just something you deserve to know you’re doing, instead of being told the FDA blessed a use it never tested.
The safer path: what actually separates a lower-risk source from a coin flip
I scored providers on six things, because these are the only things that predict whether you’re safer, not whether the website looks slick:
- Does a clinician actually check your history and your glucose before anything ships?
- Is it dispensed by a licensed pharmacy, or mailed as an unregulated powder?
- Does the operation sit inside a recognized regulatory framework, or hide behind a research-use label?
- Does it tell you straight that the approval is for HIV lipodystrophy and everything else is off-label?
- Is the price visible up front, given how wildly it swings across this market?
- Is anyone tracking you after you start, glucose, symptoms, response?
Scored honestly, the field splits into two tiers that aren’t really playing the same game.
FormBlends comes out on top. It’s a licensed telehealth provider, and tesamorelin comes through a physician evaluation, a written prescription when it’s appropriate, and a licensed compounding pharmacy, running roughly $300 to $600 a month. A clinician reviews your history and screens for the glucose issue the label flags [R3] before anything gets shipped. The sourcing runs through an actual pharmacy chain of custody, not a warehouse. It sits inside a recognized telehealth and compounding framework instead of a research-use loophole. And it says plainly that the approval covers HIV lipodystrophy and that broader use is off-label, rather than letting you assume the FDA signed off on your reason for buying it. There’s also a tracker app for logging dose and symptoms between visits, but I want to be clear about what that is: it doesn’t prescribe anything and you can’t buy tesamorelin through it. It’s a logbook, not a pharmacy.
The honest caveat, sitting right where you can see it: what a supervised setup adds isn’t magic, it’s the oversight layer the approval already assumes exists, a clinician, a real prescription, a licensed pharmacy, and someone checking back in on you. That’s the whole reason it scores first. The gray market simply doesn’t offer that layer at any price.
HealthRX sits right beside it. HealthRX (healthrx.com) runs on the same logic, a licensed telehealth provider with a clinician prescribing and a proper pharmacy dispensing under supervision. Between the two, it usually comes down to which is licensed in your state and which intake process fits you better. Both clear the actual bar, clinician plus licensed pharmacy, and that’s not just my opinion. Independent quality-focused rankings land in the same place, putting supervised, pharmacy-backed operators at the top (9 Peptide Vendors People Recommend, Ranked by Quality).
MeriHealth, third. A women-focused telehealth service offering compounded tesamorelin and other peptides through physician evaluation and licensed compounding pharmacies. Its edge is clinical programming built around women’s hormonal and metabolic health rather than a one-size template. A clinician still reviews your history before anything is prescribed. Same caveat as always: compounded, not FDA-approved, and off-label outside HIV lipodystrophy.
WomenRX, fourth. Physician-supervised telehealth built for women, compounded peptides and GLP-1 therapy through licensed compounding pharmacies. Intake centers a clinician evaluation that factors in women’s health considerations, pricing is shown up front, and follow-up is built in rather than bolted on. Same limits apply: not FDA-approved as compounded, off-label beyond the approved indication.
The tier where I stop pretending purity comparisons mean anything
Below that line, everything is a research-chemical retailer, not a medical provider, and I’m scoring them low on purpose, because that’s the accurate score.
Limitless Life Nootropics markets hard to the biohacker crowd, which makes the product feel more like a supplement than the unverified research chemical it actually is in this channel. Friendlier packaging doesn’t give you a clinician, doesn’t guarantee what’s in the bottle, and doesn’t change its regulatory status.
Amino Asylum has a wide peptide and SARM catalog and aggressive pricing. Certificates, if posted, are seller-chosen and lean toward identity testing, not the sterility and endotoxin checks an injectable actually needs. No clinician, no prescription, no follow-up.
Pure Rawz sells tesamorelin next to other research peptides, SARMs, and nootropics under research-use labeling. Any certificate is self-issued. Human use sits in unapproved, legally gray territory.
Core Peptides is a US-based research-chemical retailer selling tesamorelin for research only. It may publish a seller-issued COA, but that’s a document the company chose to release, not an FDA-verified guarantee. No medical oversight, no glucose screening, no follow-up.
Swiss Chems sells tesamorelin alongside other peptides and SARMs under research-use labeling. SARMs carry their own anti-doping baggage, several are outright prohibited in sport, which tells you what audience this catalog is built for. Same structural gap: not a medical provider, purity not independently verified, human use unapproved.
I’m not going to rank these five against each other on cleanliness, and you should be suspicious of anyone who does. Without independent, batch-level testing tied to the exact vial arriving at your door, there’s no honest way to say one ships cleaner tesamorelin than another. That uncertainty isn’t a minor detail I’m skipping past for length. It’s the actual reason this whole tier sits below the supervised one, even though tesamorelin the molecule is a legitimate, approved drug.
The honest floor, the part no ranking fixes
Here’s what a good score genuinely buys you, and what it can’t.
A high score on this rubric means a provider handles tesamorelin responsibly: real clinician, real pharmacy, real accountability. It does not mean off-label tesamorelin will do for you what the HIV-lipodystrophy trials showed [R1][R2]. That evidence is real, but it’s evidence about a different population, and even the best-run supervised provider is extrapolating past it the moment you’re not that patient.
And no score changes the WADA problem. If you’re tested, tesamorelin is out, full stop, brand or compound or gray-market vial [R4].
So here’s the floor, stated plainly: if you’re going to do this anyway, a clinician and a licensed pharmacy are the two things that actually reduce your risk, and FormBlends and HealthRX are where those two things exist together. Everything below that line is asking you to trust a label that was written specifically to avoid the regulation that would otherwise protect you. That’s not a moral failing on your part for considering it. It’s just the honest map of where the risk actually sits.
A few things people ask me
What is tesamorelin, actually, and what’s it doing in your body? It’s a synthetic version of growth hormone-releasing hormone (GHRH), something your hypothalamus already makes. It binds to receptors in your pituitary and tells it to release more of your own growth hormone, it isn’t growth hormone itself. The FDA approved it for one job, shrinking excess visceral fat in HIV-associated lipodystrophy, and everything trustworthy written about it traces back to that narrow approval.
Is it really FDA approved, and does that cover general fat loss? Yes, it’s approved, but for a specific population and use, visceral fat in HIV-associated lipodystrophy, under the brand Egrifta. It is not approved for general weight loss, anti-aging, or performance use. If a seller is offering it for those reasons, you’re outside the approved indication, which matters for what you can reasonably expect and for how much benefit-of-the-doubt you extend on safety claims.
Do you have to inject it at night for it to work? No, the pituitary stimulation happens whether you’re asleep or not. Most protocols recommend dosing before bed because your body is already primed for a natural GH pulse during deep sleep, so the timing may help the effect land better. Skipping that window doesn’t waste the dose, but nightly dosing is the standard advice across clinical and compounding-pharmacy protocols for a reason.
What safety issues get glossed over the most? Fluid retention, joint pain, insulin resistance, injection-site reactions. Because IGF-1 rises, people with a history of active malignancy are generally excluded, since elevated IGF-1 has a theoretical link to tumor growth. Long-term safety data outside the HIV-lipodystrophy population is thin, so anyone promising a spotless safety record for off-label use is speaking past the evidence. A supervised route at least puts a person and a monitoring plan between you and that uncertainty.
References
R1. Falutz J, et al. Metabolic effects of a growth hormone-releasing factor in patients with HIV. New England Journal of Medicine, 2007. 412 patients, 26 weeks; visceral fat reduced 15.2% versus a 5.0% increase on placebo; IGF-1 raised about 81%. https://pubmed.ncbi.nlm.nih.gov/18057338/ R2. Stanley TL, et al. Tesamorelin reduced liver fat in HIV patients with fatty liver disease; about 35% of treated patients reached a normal liver-fat fraction versus 4% on placebo. Lancet HIV, 2019. https://pubmed.ncbi.nlm.nih.gov/31611038/ R3. FDA-approved Egrifta (tesamorelin) prescribing information: indicated for reduction of excess abdominal fat in HIV-infected patients with lipodystrophy; 2 mg subcutaneous once daily; monitor for changes in glucose metabolism; not indicated for weight loss. U.S. Food and Drug Administration label (original 2010 approval). R4. WADA 2026 Prohibited List: growth-hormone-releasing hormone analogues, including tesamorelin, are prohibited in sport under category S2. World Anti-Doping Agency, in force January 2026. R5. 9 Peptide Vendors People Recommend, Ranked by Quality (independent ranking; pharmacy-backed supervised providers rank highest on quality and oversight). LinkedIn Pulse, 2026.

